MBCT combines mindfulness and cognitive therapy to treat depression and anxiety. Learn how it works, the 8-week programme, and how it differs from CBT and standard mindfulness.
MBCT — Mindfulness-Based Cognitive Therapy — is one of the most thoroughly researched psychological treatments of the past three decades. Developed in the 1990s by Zindel Segal, Mark Williams, and John Teasdale, it has since been endorsed by the National Institute for Health and Care Excellence (NICE) as a first-line treatment for recurrent depression, and has been shown in multiple randomised controlled trials to reduce the risk of depressive relapse by up to 43 per cent. It is now delivered in NHS trusts, university clinics, schools, and private practices across the world.
But the technical evidence does not fully capture what makes MBCT remarkable. The insight at its heart — that our relationship to our thoughts matters far more than the content of those thoughts — is as applicable in a mindfulness retreat in rural Wales as it is in a clinical group in an NHS waiting room. This guide covers what MBCT is, how it works, what the research shows, and how to find a programme that is right for you or your family.
The short answer
MBCT is a structured 8-week group programme that combines mindfulness meditation with cognitive therapy principles to prevent depression from recurring. It is recommended by NICE, as effective as antidepressants for relapse prevention in clinical trials, and available on the NHS. It works not by changing what you think, but by changing your relationship to thinking itself.
What does MBCT stand for?
MBCT stands for Mindfulness-Based Cognitive Therapy. The name tells you everything you need to know about its construction: it is mindfulness (the deliberate, non-judgemental observation of present-moment experience) layered on top of cognitive therapy (the understanding that patterns of thinking drive patterns of mood).
The key insight is this: you do not need to change your thoughts in order to change how they affect you. You need to change your relationship to them. When you can observe "I always fail" as a thought arising in awareness — a mental event rather than a statement of fact — it loses much of its power to trigger the cascade of low mood, withdrawal, and hopelessness that characterises depression.
This sounds simple. It is not easy. Learning to observe thought rather than inhabit it is a genuine skill that takes practice — which is exactly what the 8-week programme provides.
The problem MBCT was designed to solve
Segal, Williams, and Teasdale were not trying to build a new mindfulness programme. They were investigating a specific clinical problem: why does depression recur?
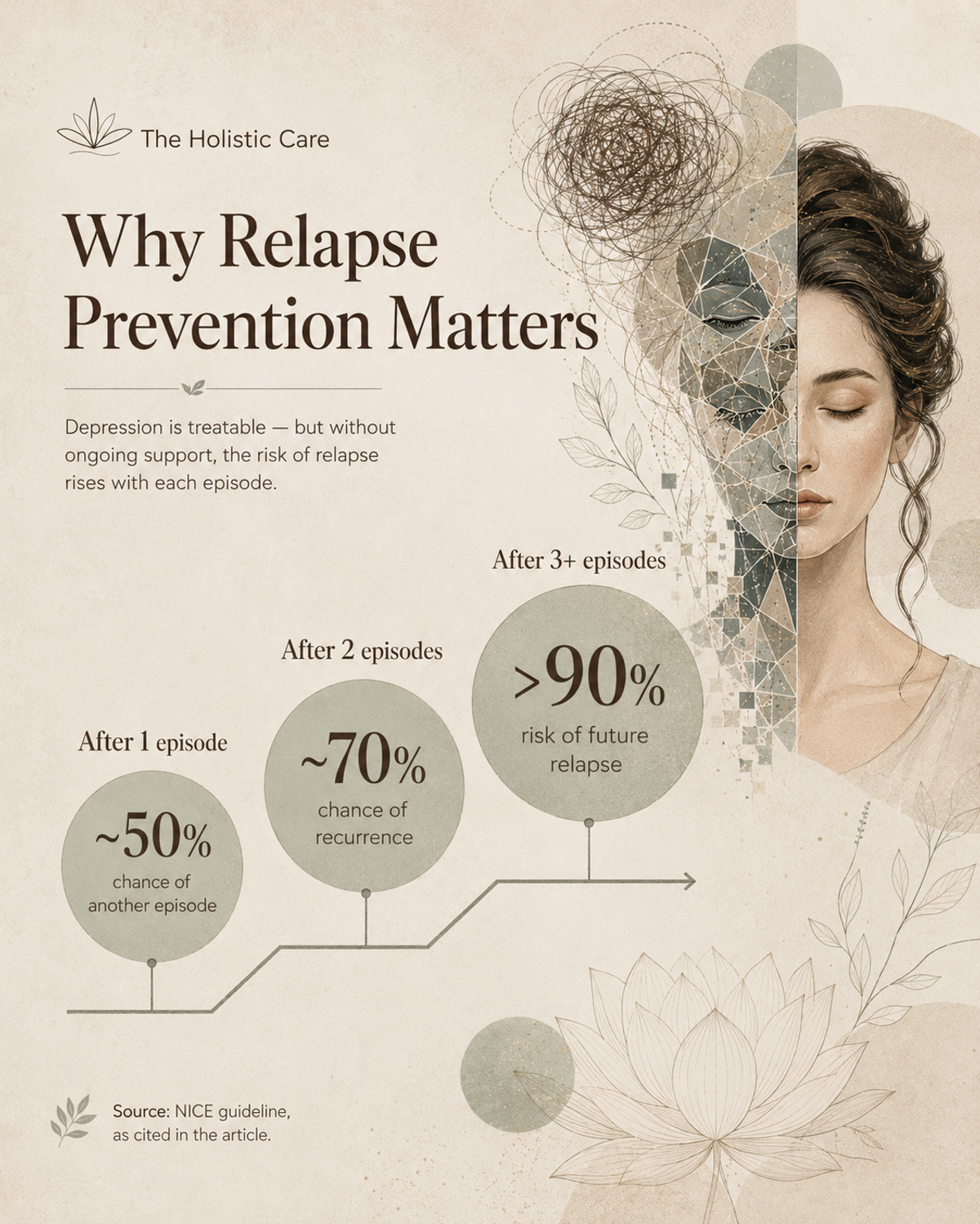
They had observed something puzzling. People who had recovered from one episode of depression were far more likely to have another — and with each episode, the threshold for relapse lowered. After one episode, the chance of a second is roughly 50 per cent. After two, it rises to 70 per cent. After three or more, it exceeds 90 per cent. (Source: NICE guideline CG90.) Something was making the brain progressively more vulnerable.
The answer they identified was cognitive reactivity. In people with a history of depression, even mild low mood — the kind everyone experiences occasionally — reactivates the same patterns of negative thinking that characterised their previous episodes. The brain has learned, through repetition, to link ordinary sadness with a cascade of catastrophic thought: "I am worthless, nothing will ever improve, I cannot cope." Ordinary mood becomes a trigger for clinical depression.
CBT offered one solution: change the content of those thoughts, challenge the distortions, find more balanced alternatives. But Segal, Williams, and Teasdale had a more radical idea. What if patients did not need to change their thoughts at all? What if they could learn to relate to them differently — to notice the cascade beginning, to step back from it, and to watch it pass without being swept away?
That is the central mechanism of MBCT. And it is why the programme teaches mindfulness: not as a relaxation technique (though it often relaxes), but as a precision tool for changing your relationship to your own mind.
"The goal of MBCT is not to feel good. The goal is to see clearly — to observe the mind's movements without being driven by them. From that observational stance, much of the suffering that depression produces simply does not arise."
How MBCT works: the mechanism
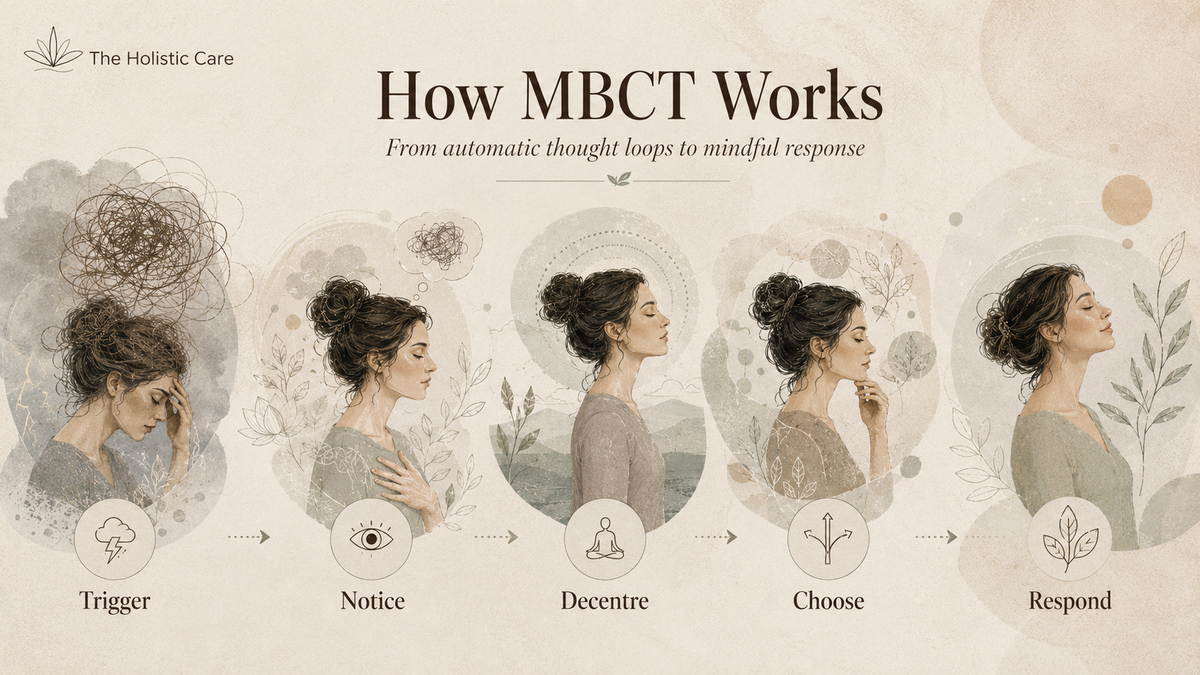
MBCT operates through a mechanism called decentring — the capacity to observe your own thoughts and feelings from a slight distance, as transient mental events rather than fixed truths. In clinical language, decentring is the opposite of cognitive fusion: instead of being fused with your thoughts (believing them automatically and acting from them), you can see them as thoughts.
Here is what this looks like in practice. A person with a history of depression wakes up feeling flat on a grey morning. Without MBCT, that flat feeling tends to trigger a chain of automatic thinking: "Why do I feel this way? There must be something wrong with me. I am never going to feel better. I can't cope with today." Each thought feels like a fact. The chain gains momentum, mood drops further, motivation collapses, and the person withdraws — confirming the thought that they cannot cope.
With MBCT training, the same flat feeling arises. But instead of being instantly swept into thought, the person has learned to notice: "There is a feeling of flatness. Thoughts are arising about why this might be. I am beginning to think I cannot cope." The observing — the act of noticing — creates a gap between feeling and reaction. In that gap, a different response becomes possible. The person can choose to act on what matters to them, rather than on the content of the thought.
This is not suppression. The thoughts still arise. The feelings are still felt fully. What changes is the automatic, reflexive identification with them — the assumption that thought equals truth.
The neuroscience behind MBCT
Brain imaging research has begun to map the neurological changes that MBCT produces. While caution is always warranted in translating neuroscience to clinical claims, several findings are consistent and replicated.
Mindfulness practice — the core skill of MBCT — has been shown to reduce activity in the default mode network (DMN), the neural system responsible for mind-wandering, self-referential thinking, and rumination. High DMN activity correlates strongly with depression and anxiety. MBCT-trained individuals show reduced DMN activity even outside formal meditation, suggesting a lasting change in default cognitive patterns rather than a state that exists only during practice.
MBCT also appears to strengthen the prefrontal cortex's regulation of the amygdala — the brain's threat-detection centre. In depression and anxiety, the amygdala is hypersensitive, triggering threat responses to neutral or ambiguous stimuli. Mindfulness training increases the cortical brake on this response, reducing emotional reactivity without numbing emotional experience.
Research by Farb et al. (2010) found that MBCT training shifted neural processing from a narrative, self-evaluative mode (associated with rumination) to an experiential, present-moment mode. This corresponds exactly to the clinical mechanism described above: less time spent in the story of self, more time in direct experience.
Neurological changes documented in MBCT research
Reduced DMN activity
Less rumination and self-referential mind-wandering — the neural signature of depression
Stronger PFC-amygdala regulation
Greater emotional regulation without suppression — responding rather than reacting
Increased insula activity
Greater interoceptive awareness — noticing body sensations before they become overwhelming
Narrative → experiential mode shift
Less time in the story of self; more time in direct present-moment experience (Farb et al., 2010)
MBCT vs CBT vs MBSR: what is the difference?
People often confuse MBCT with CBT (cognitive behavioural therapy) and MBSR (mindfulness-based stress reduction). They share roots but serve different purposes.
| Approach | Core mechanism | Primary use | Format | Evidence base |
|---|---|---|---|---|
| MBCT | Change relationship to thought; decentring | Recurrent depression relapse prevention | 8-week group programme | NICE-endorsed; 43% relapse reduction |
| CBT | Change the content of unhelpful thoughts | Active depression, anxiety, OCD, phobias | Individual sessions (12–20 typical) | NICE-endorsed; gold standard for many conditions |
| MBSR | Present-moment awareness; stress reduction | General wellbeing, chronic pain, stress | 8-week group programme + 1 full day | Extensive; not a clinical programme |
| DBT | Distress tolerance, emotional regulation | Borderline personality, chronic self-harm | Intensive individual + group | Strong evidence for BPD specifically |
The most important distinction for most people: if you are currently in an active depressive episode, MBCT is not the right starting point. It requires enough mental bandwidth to engage with meditation and group work. CBT or medication are better acute-phase treatments. MBCT is for when you have recovered — and want to stay recovered.
The MBCT 8-week programme: what happens each week
MBCT is delivered as a group programme with 8–15 participants and one or two trained facilitators. Sessions run for approximately two hours each week, and daily home practice (30–45 minutes) is expected between sessions. The programme follows a specific arc.
Each session follows a rhythm: a guided meditation practice, inquiry into participants' experience of home practice, psychoeducation about a specific cognitive or emotional pattern, and discussion of how the learning applies in daily life. The facilitator does not give advice. They facilitate inquiry — helping participants discover their own patterns rather than being told what those patterns are.
What does an MBCT session actually feel like?
Many people arrive at their first MBCT session expecting something resembling a therapy group — talking about their problems, receiving guidance, perhaps crying. What they find is different.
The session typically begins with a 20-minute guided meditation. You sit — on a chair, not necessarily on the floor — and the facilitator guides your attention through a body scan or a breathing awareness practice. You are not asked to relax, to think positively, or to achieve any particular state. You are asked to notice whatever is actually present: sensations in the body, the movement of breath, the arising of thoughts and feelings — and to gently return attention to the present moment whenever it wanders.
Then there is inquiry: the facilitator asks what participants noticed, what was easy or difficult, what arose. This is not therapy in the usual sense — there is no analysis, no interpretation, no advice. The facilitator holds a space in which participants discover their own patterns. This process is itself a model of the decentring skill that MBCT teaches.
The group format matters. Hearing others describe experiences similar to yours — the mind wandering compulsively, the difficulty sitting with discomfort, the judgement that arises about one's own meditation — normalises the experience and reduces shame. Research suggests that the group context contributes meaningfully to MBCT outcomes, beyond what the meditation practice alone produces.
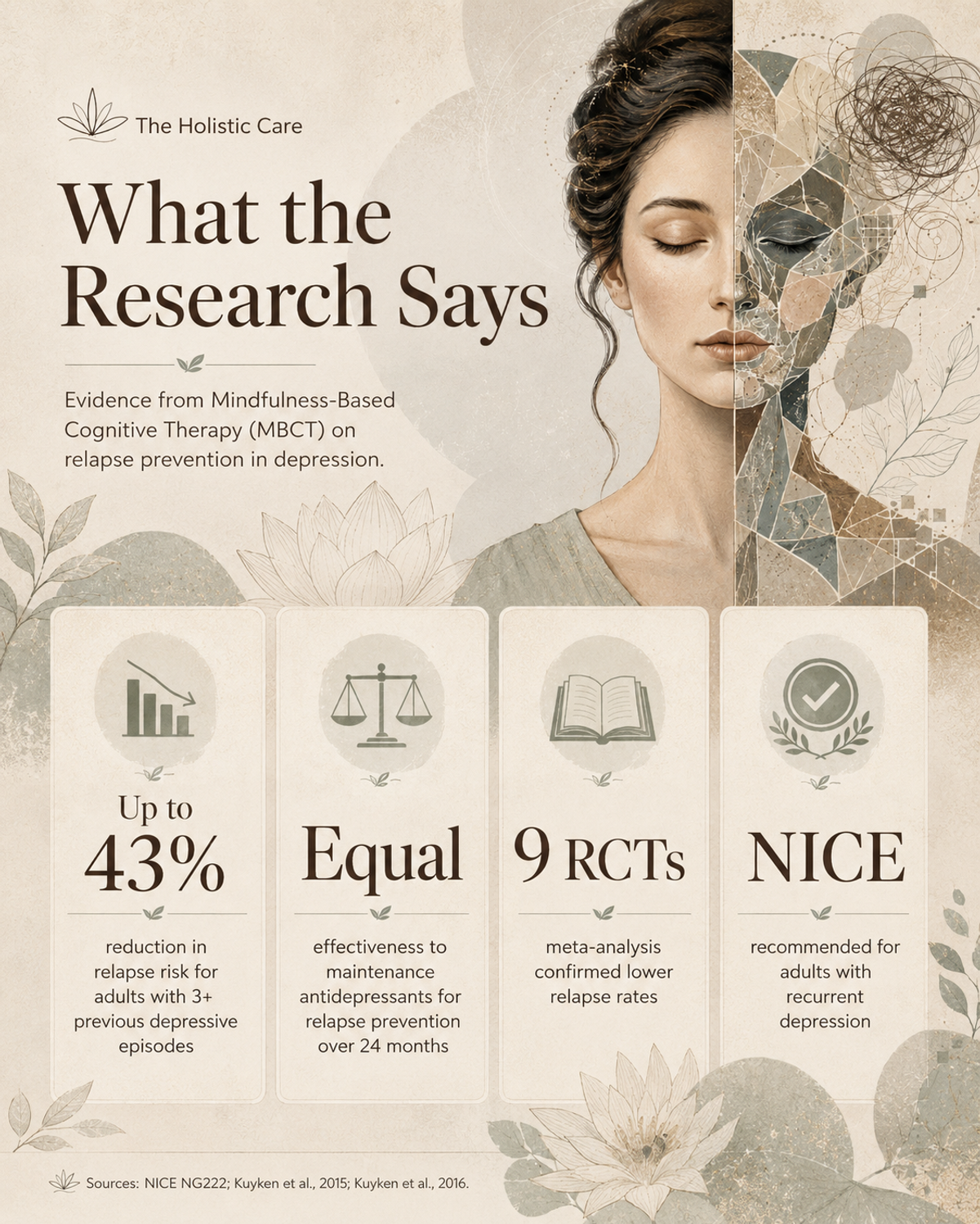
What does the research say about MBCT?
The evidence base for MBCT is one of the strongest for any psychological intervention developed in the past 30 years. The headline findings are robust, replicated, and have withstood considerable scientific scrutiny.
43%
Reduction in relapse risk for adults with 3+ previous depressive episodes (Teasdale et al., 2000; Ma & Teasdale, 2004)
Equal
Effectiveness to maintenance antidepressants for preventing depressive relapse (Kuyken et al., 2015, LANCET)
9 RCTs
Meta-analysis confirming MBCT significantly reduces relapse rates — effect strongest in those with highest residual symptoms (Kuyken et al., 2016)
NICE
UK national clinical guideline endorses MBCT for adults with 3+ depressive episodes — one of only two psychological treatments to receive this status
The 2015 Kuyken et al. landmark trial published in The Lancet is particularly significant: it compared MBCT plus support to taper antidepressants against maintenance antidepressant treatment alone, and found MBCT equally effective at preventing relapse over a 24-month follow-up period. Critically, MBCT offered this protection even for patients who successfully came off antidepressants — a finding with significant implications for the millions of people who wish to reduce long-term medication use with appropriate support.
Research has also demonstrated MBCT's effectiveness for anxiety. Specifically, MBCT reduces generalised anxiety disorder symptoms, health anxiety, and worry — the rumination-heavy thought patterns that share a cognitive mechanism with depression.
For bipolar disorder, MBCT has been evaluated as an adjunct to medication, with positive findings for reducing depressive symptoms and increasing wellbeing. It is not a standalone treatment for bipolar disorder.
Who is MBCT for?
MBCT has the strongest evidence base for one specific population: adults who have recovered from recurrent major depression (three or more previous episodes) and want to reduce their risk of relapse. NICE recommends it for exactly this group.
Beyond this core application, MBCT is now used for:
- Generalised anxiety disorder and worry — the core decentring skill directly addresses the rumination loops that maintain anxiety
- Residual depressive symptoms — MBCT is particularly effective for people who have recovered from depression but still experience persistent low-level symptoms
- Bipolar disorder — as an adjunct to medication, to increase wellbeing and reduce depressive relapse between episodes
- Chronic pain — changing the relationship to pain rather than trying to eliminate it produces meaningful reductions in suffering
- Eating disorders — specifically binge eating, where the decentring skill interrupts the automatic chain from distress to eating
- Health anxiety — MBCT reduces the catastrophic interpretation of physical sensations that drives health anxiety
- Workplace stress and burnout — adapted MBCT-informed programmes are widely used in healthcare, education, and corporate settings
When MBCT is NOT the right choice
MBCT is not suitable for everyone. Being clear about this is important — recommending MBCT to someone who needs a different intervention can delay appropriate help.
MBCT is generally not appropriate for people currently in an acute depressive episode. The cognitive demands of group work, daily home practice, and mindfulness meditation are beyond what most people can manage when acutely depressed. Acute episodes typically require medication, intensive individual therapy, or both. MBCT is for after recovery, not during it.
MBCT may also not be suitable for people with severe trauma who have not had prior trauma-specific therapy. Body-based mindfulness practices can be dysregulating for trauma survivors without prior stabilisation work. Specialist trauma-informed MBCT adaptations exist, but should only be delivered by therapists with explicit trauma training.
People with active psychosis, current severe self-harm, or active suicidal ideation need crisis-appropriate support before considering MBCT. Similarly, substance dependence that is currently active needs specialist addiction support first.
Seek specialist guidance first if you have
Active depressive episode · Severe unprocessed trauma · Active psychosis · Current suicidal ideation · Severe active addiction · Acute crisis of any kind
MBCT vs antidepressants: what the evidence actually shows
One of the most frequently asked questions about MBCT is how it compares to antidepressant medication. The short answer is: for relapse prevention in recurrent depression, MBCT is as effective as maintenance antidepressants, with some important caveats.
The 2015 Kuyken et al. Lancet trial found that MBCT plus support to taper medication was not inferior to maintenance antidepressants for preventing relapse over two years. A 2016 meta-analysis by the same team, covering data from 1,258 patients across nine studies, confirmed this finding. MBCT performed best for patients with the most severe residual depressive symptoms — the group at highest relapse risk.
These findings do not mean that MBCT is better than medication, or that people should stop taking antidepressants in favour of MBCT. They mean that MBCT provides a viable evidence-based alternative for people who have recovered from recurrent depression and wish to reduce long-term medication use. This should always be done with medical supervision.
For acute depression, antidepressants remain a first-line treatment with a much stronger evidence base than MBCT. MBCT is not an acute treatment. Using it as a replacement for medication during an active episode is not supported by the research and could cause harm.
Online MBCT vs in-person: does it work online?
Access to in-person MBCT has historically been limited by geography, cost, and waiting times. The COVID-19 pandemic accelerated the development of online MBCT programmes, and the evidence has largely been positive.
A 2021 systematic review found online MBCT programmes (both live video-based and self-paced digital formats) produced comparable reductions in depression and anxiety to in-person delivery. The group dynamic — often assumed to be critical — appears to translate surprisingly well to online formats. The OMindful programme, developed by the Oxford Mindfulness Foundation, and the Be Mindful digital programme have both been evaluated in clinical research with positive findings.
The main advantage of online delivery is access: programmes are available to people in areas with no local MBCT practitioners, to those with mobility limitations, and to those who cannot commit to a fixed weekly venue. The main limitation is that some participants find the informal contact between group members (chatting before sessions, connecting after) harder to achieve online — and this informal contact appears to contribute to outcomes.
For most people, the best MBCT is the MBCT they can actually access and consistently attend. If in-person is available and practical, it is slightly preferred. If it is not, online is a genuine and well-evidenced alternative.
MBCT for children and young people
Growing evidence supports the adaptation of MBCT principles for children and adolescents — not for relapse prevention in the clinical sense, but for the same underlying skills: observing thoughts without fusing with them, recognising emotional escalation early, and developing a stable relationship with present-moment awareness.
For adolescents, the relevance is particularly clear. Adolescence is characterised by an intensification of self-monitoring — the constant evaluation of how I appear, whether I measure up, whether I belong. These are not pathological thoughts; they are developmentally normal. But in young people who are prone to depression or anxiety, these same thoughts become the engine for clinical distress. MBCT-informed practices offer a tool for observing the monitoring process without being driven by it.
Adapted youth programmes typically involve shorter sessions (45–60 minutes), more movement-based practices, age-appropriate metaphors, and less emphasis on home practice. Research supports their effectiveness: Cotton et al. (2016) found significant reductions in anxiety and depressive symptoms in adolescents, and Chi et al. (2018) found mindfulness-based interventions produced sustained reductions in anxiety and depression across multiple studies.
At The Holistic Care
Our programmes for children and young people aged 4–18 draw on the same foundational insight as MBCT — that there is an aware presence beneath all thought and emotion that is not disturbed by either — and root it in the Advaita Vedanta tradition alongside contemporary mindfulness science. Our I AM programme for schools integrates this contemplative understanding into school-based delivery, complementing MBCT-informed approaches particularly well. Learn about the I AM programme →
The deeper dimension: MBCT and nondual awareness
MBCT derives its clinical mechanics from secular Western psychology. But the insight at its core — that there is an observing awareness that is not disturbed by the thoughts passing through it — has far deeper roots. Every contemplative tradition that has investigated the nature of mind has pointed to the same discovery: thoughts, feelings, and sensations arise and pass within awareness, but awareness itself remains undisturbed.
In the Advaita Vedanta tradition — the non-dual school of Hindu philosophy — this undisturbed awareness is understood not as a skill to be developed but as the fundamental nature of what you already are. The "decentring" that MBCT teaches is, from this perspective, not a technique for managing mental illness. It is a glimpse of what is always already the case.
At The Holistic Care, our approach to mindfulness education begins from this deeper understanding. We use MBCT-derived practices as an accessible entry point — secular, evidence-based, recognisable to schools and healthcare systems. But we do not end there. The I AM programme, the Still the Storm adult course, and the Calm the Storm children's curriculum all point towards the same recognition that MBCT glimpses: that there is a presence beneath thought that is already whole.
This is not a rejection of MBCT's clinical value. It is an acknowledgement that the healing MBCT facilitates is a doorway to something larger — and that clients and students who encounter that larger understanding often find their need for therapeutic maintenance diminishes substantially.
Featured Programme
The I AM Programme for Adults
A 7-week nondual mindfulness course grounded in Advaita Vedanta — for those who want to take the insight behind MBCT all the way to its source. Suitable after or alongside MBCT for those drawn to explore the nature of awareness itself.
Explore the I AM Programme →How to find an MBCT programme
NHS and public health services (UK)
MBCT is available through NHS IAPT (Improving Access to Psychological Therapies) services. Ask your GP for a referral, or self-refer through your local IAPT service — most areas now accept self-referral. Waiting times vary but typically range from 4–16 weeks. NHS MBCT is typically delivered in groups of 8–15 people.
Private MBCT practitioners
For faster access, look for practitioners accredited by the British Association for Mindfulness-Based Approaches (BAMBA) at bamba.org.uk. BAMBA accreditation requires practitioners to have completed an approved teacher training programme, attended their own retreat, and received supervision. This is the most reliable quality indicator for MBCT practitioners in the UK.
Online MBCT programmes
The Oxford Mindfulness Foundation offers online and in-person programmes. Be Mindful (bemindful.co.uk) provides a validated digital MBCT course available immediately. Both have research evidence behind them. For a guided self-paced option, the Frantic World website by Williams and Penman (the popular version of MBCT) offers resources that complement the programme.
International options
In Australia, the Centre for Mindfulness at Monash University and the Centre for Mental Health at Melbourne University offer programmes. In the United States, look for practitioners affiliated with the Association for Mindfulness-Based Approaches (AMBA) or the UC San Diego Center for Mindfulness. In Canada, the University of Toronto Mindfulness Studies programme trains practitioners whose clients can be found through professional directories.
How to prepare for your first MBCT session
MBCT works best when you come with openness rather than expectations. Specifically:
- Commit to the daily practice. The research evidence for MBCT is built on programmes where participants practised 30–45 minutes daily. Evidence shows that home practice predicts outcomes more strongly than attendance alone. If you attend all eight sessions but do minimal practice between them, the outcomes are significantly reduced.
- Expect discomfort. Turning attention towards difficult thoughts and feelings — rather than away from them — is uncomfortable, at least initially. This is not a sign that something is wrong. It is a sign that the practice is working.
- Don't try to achieve a state. Many people arrive expecting MBCT to make them relaxed, peaceful, or calm. This may happen. But relaxation is not the goal. Noticing — whatever is present — is the goal. Paradoxically, people who try less hard to feel calm often experience more calm.
- Tell your GP or psychiatrist you are starting. If you are on antidepressants, do not change your medication without medical advice. MBCT is not a substitute for medication unless specifically agreed with your prescriber.
- Bring a beginner's mind. The concept of "beginner's mind" — approaching each moment as if for the first time — is one of the attitudes cultivated in MBCT. Starting the programme itself with this attitude tends to produce better outcomes than starting with strong preconceptions about what mindfulness is or is not.
Also Explore on The Holistic Care
- → MBCT for Children and Young People
- → Mindfulness for Anxiety: Evidence-Based Techniques
- → 25 Mindfulness Techniques: A Complete Toolkit
- → Mindfulness Exercises: 20 Simple Practices for Daily Life
- → How to Meditate: A Beginner's Complete Guide
- → All Mindfulness Courses
- → Mindfulness in Schools Programmes
- → Corporate Wellness & Workplace Mindfulness
Frequently asked questions about MBCT
What does MBCT stand for?
MBCT stands for Mindfulness-Based Cognitive Therapy. It is a structured 8-week psychological programme developed in the 1990s by Zindel Segal, Mark Williams, and John Teasdale. It combines mindfulness meditation practices with cognitive behavioural therapy principles, and was originally designed to prevent recurrent depression from recurring.
Does MBCT work for anxiety?
Yes. While MBCT was developed specifically for recurrent depression, research supports its effectiveness for generalised anxiety disorder, health anxiety, and worry. The core mechanism — observing anxious thoughts without fusing with them — directly addresses the rumination loops that maintain anxiety. Several meta-analyses have found significant anxiety reductions in MBCT programmes.
How long does MBCT take to work?
Most participants notice changes during the programme — typically from around weeks 3–5. Sustainable changes in cognitive patterns typically consolidate over 3–6 months of continued practice after the programme ends. The research evidence for relapse prevention is based on follow-up periods of 12–24 months, suggesting that effects strengthen with continued practice.
Is MBCT available on the NHS?
Yes. NICE guidelines recommend MBCT for adults who have had three or more depressive episodes, and it is available through IAPT services across the UK. You can ask your GP for a referral, or self-refer through your local IAPT service. Waiting times vary by area, typically from 4–16 weeks.
Can MBCT be done online?
Yes. Research supports the effectiveness of online MBCT delivered via live video group sessions. Self-paced digital programmes have also been validated in clinical research. The Oxford Mindfulness Foundation and Be Mindful are the most thoroughly researched digital options available in the UK.
What is the difference between MBCT and CBT?
CBT works to identify and change the content of unhelpful thoughts — examining the evidence, finding more balanced alternatives. MBCT does not try to change thoughts. It teaches a different relationship to them: observing thoughts as mental events rather than facts, without trying to alter their content. CBT is often used during an active depressive episode; MBCT is designed primarily for relapse prevention after recovery.
Can children do MBCT?
Adapted versions of MBCT are used with children from around age 7–8 upwards. Programmes for children are shorter (45–60 minutes), use age-appropriate language, include more movement, and reduce home practice expectations. For children under 7, general mindfulness practices are more appropriate. The adolescent adaptation (MBCT-A) is designed specifically for ages 13–17 and follows the same core structure as adult MBCT.
What is cognitive reactivity, and why does it matter for MBCT?
Cognitive reactivity is the tendency for mild low mood to automatically reactivate the negative thought patterns associated with previous depressive episodes. Research by Teasdale and colleagues found that cognitive reactivity — not ongoing life stress — is the primary predictor of depressive relapse. MBCT directly targets cognitive reactivity by training the decentring capacity: the ability to notice thought patterns arising without being automatically drawn into them.
How is MBCT different from standard mindfulness?
Standard mindfulness — as taught in MBSR (Mindfulness-Based Stress Reduction) — builds present-moment awareness as a general skill. MBCT is more targeted: it combines mindfulness with explicit psychoeducation about depression — how it works, what triggers relapse, and how to interrupt the cognitive patterns that maintain it. MBCT is a clinical programme; mindfulness is a broader practice. You can benefit from mindfulness without MBCT, but MBCT without mindfulness is not possible.
Is MBCT a replacement for antidepressants?
For people with recurrent depression who have recovered and wish to reduce medication, MBCT provides an evidence-based option for doing so with support. The 2015 Kuyken et al. Lancet trial found MBCT plus supported medication tapering was as effective as maintenance antidepressants over two years. This should always be done in consultation with a GP or psychiatrist. MBCT is not appropriate as a replacement for medication during an active depressive episode.
What training should an MBCT teacher have?
In the UK, look for practitioners accredited by the British Association for Mindfulness-Based Approaches (BAMBA) at bamba.org.uk. BAMBA accreditation requires completion of an approved 200+ hour teacher training programme, personal attendance at an 5+ day silent retreat, and ongoing supervision. This level of training is associated with significantly better client outcomes than unaccredited instruction. Outside the UK, look for practitioners trained by recognised university centres such as Oxford, Bangor, or UCSD.
What happens if I find MBCT difficult?
Finding MBCT difficult is normal and, to a degree, expected. The practices deliberately invite attention towards discomfort rather than away from it — which is uncomfortable. The key is to distinguish between the productive discomfort of genuine practice (feeling frustrated with a wandering mind, noticing that sitting with difficult emotions is hard) and a reaction that suggests the programme is not appropriate (dissociation during meditation, strong trauma responses, significant deterioration in wellbeing). Talk to your facilitator if you are unsure. Good MBCT facilitators are trained to respond to difficulty, adjust practices, and refer on when needed.

Written by
Mohan ChuteHead of Marketing & AI Strategy | Digital Transformation Leader | Nonduality Mindfulness Teacher | Author | Explorer of Consciousness
Mohan Chute is a rare blend of technology strategist and mindfulness teacher. With over 23 years of experience in digital marketing, AI strategy, and growth leadership, he has guided organizations through automation, analytics, branding, and digital transformation. Alongside this professional expertise, Mohan has devoted his life to exploring meditation, yoga, and nondual awareness—helping people discover balance, presence, and authenticity in a fast‑paced world.
💻 AI & Digital Expertise
As a strategist and innovator, Mohan empowers businesses to harness AI, automation, and analytics to drive growth. His leadership in go‑to‑market strategy, branding, and digital transformation positions him at the forefront of innovation—while keeping human wellbeing at the center.
🧘♂️ The Journey Within
At 17, Mohan discovered meditation on his own—a spark that ignited a lifelong journey into yoga, mindfulness, and nondual inquiry. Today, he integrates this wisdom into both personal and professional domains, showing that technology and consciousness can coexist to create meaningful impact.
🌍 Founder & Teacher
Through The Holistic Care Foundation, Mohan leads transformative programs worldwide. His Nonduality & Mindfulness‑based education initiatives support schools, colleges, and communities in cultivating calm, connected, and compassionate learning environments. For corporate teams, his programs position mindfulness as a competitive edge—enhancing creativity, reducing burnout, and fostering resilient workplace cultures.
📚 Author of Inspiring Works
Mohan’s books span audiences from children to spiritual seekers, weaving story, metaphor, and practice into accessible journeys of awareness. His published works include:
Mindful Adventures for Little Minds
In the Garden of Kindred Spirits
The Wondrous Quest: Journey to the Knower Within
I Am – The Heart of Being
Seeds of Kindness
Mindful Computing: Embracing Presence in a Digital World
The Awareness Chronicles series:
Book 1: The Magic Sketchbook
Book 2: The Movie Projector
Book 3: The Mask Maker
Book 4: The Listening River
Book 5: The True Compass
🎓 Interactive eLearning Courses
Each of these books has been transformed into interactive eLearning programs available on The Holistic Care. These courses combine storytelling, reflection prompts, creative activities, and mindfulness practices—making awareness accessible to children, teens, educators, families, and professionals.
🌈 A Guiding Light
Whether you are a student, educator, professional, or seeker, Mohan’s voice offers clarity and compassion. His mission is simple yet profound: to help people live with balance, presence, and purpose—reminding us that awareness is not the end, but the beginning.